.png)

Your child's dentist just mentioned something called "interceptive orthodontics," and now you are wondering what it means, whether your child really needs it, and whether starting treatment so early is actually a good idea.
You are not alone. A lot of parents in Lafayette come to our office with these same questions.
Here is the short answer: interceptive orthodontics, also called Phase 1 orthodontics, is early dental treatment that guides jaw growth and corrects bite and tooth problems in children while baby teeth are still present. It typically begins between the ages of 6 and 9, long before full braces are needed. The goal is simple: catch and fix developing problems while a child's jaw is still growing and easy to guide, so those problems do not become bigger, more expensive issues later.
This guide will walk you through everything you need to know, including the full benefits of interceptive orthodontics for children, the warning signs to watch for, what treatment actually looks like, and whether it is the right choice for your child.
What Is Interceptive Orthodontics (Phase 1)? And How Is It Different from Regular Braces?
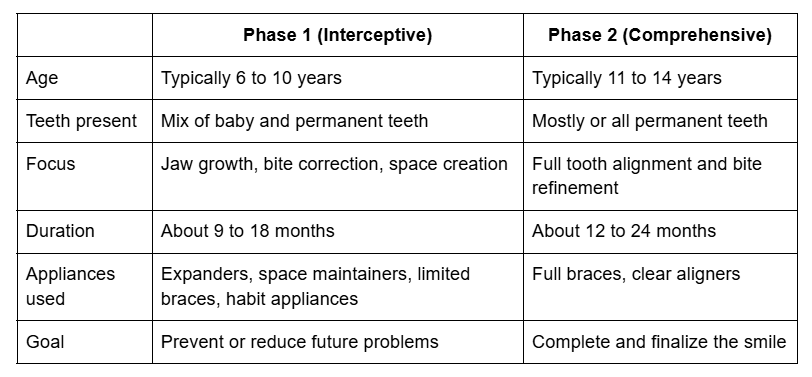
Interceptive orthodontics is not the same as the braces most of us had as teenagers. Regular braces, also called Phase 2 or comprehensive orthodontics, are used when all permanent teeth have come in, usually around ages 11 to 14. The goal at that stage is to straighten teeth and refine the bite.
Interceptive orthodontics, or Phase 1, happens much earlier. It targets the jaw structure, the bite, and the spacing of teeth while a child is still in what dentists call the "mixed dentition" phase, meaning a mix of baby teeth and permanent teeth are present. Research has shown that certain bite problems can benefit from early intervention and can help to either reduce the duration or even avoid the necessity of more substantial treatment at a later stage. (Reference)
Think of it this way: Phase 1 works with the jaw. Phase 2 works with the teeth. Both are sometimes needed, but in some children, a well-timed Phase 1 can make Phase 2 much shorter, simpler, or in some cases unnecessary altogether.
Phase 1 vs. Phase 2: A Simple Comparison
Who performs interceptive orthodontics? A trained pediatric dentist or orthodontist. At Dr. Leslie Jacobs Pediatric Dentistry in Lafayette, we evaluate children for early orthodontic issues as part of routine care because catching a problem at age 7 is far easier to address than waiting until it becomes a structural concern at age 12.
When Should a Child Start? The AAO Age 7 Rule Explained
The American Association of Orthodontists (AAO) recommends that children should get their first check-up with an orthodontic specialist at the first recognition of a developing orthodontic problem, but no later than 7 years of age.
Why age 7 specifically? By this age, a child typically has their first permanent molars and some permanent front teeth. This combination gives a dentist enough information to evaluate the bite, the jaw relationship, and whether permanent teeth have enough room to come in properly.
Importantly, an evaluation at age 7 does not mean your child will immediately start treatment. Most kids, about 90% of children, will not need early interceptive treatment. Many will simply be monitored over time. But for the children who do need early intervention, catching it at this age makes all the difference.
Signs Your Child May Need an Evaluation
As a parent, you know your child best. Here are warning signs that your child may benefit from an interceptive orthodontic evaluation:
- Teeth that appear crowded, crooked, or overlapping
- Early or unusually late loss of baby teeth (before age 5 or still present after age 13)
- Difficulty biting or chewing food properly
- Mouth breathing, snoring, or consistently breathing through the mouth
- Thumb sucking or finger sucking that continues past age 4 or 5
- Front teeth that stick out noticeably (protruding teeth)
- Upper and lower teeth that do not meet properly when biting (crossbite, underbite, or open bite)
- Jaw that shifts, clicks, or makes noise when opening or closing
- Speech issues such as a lisp
- Visible difference in the position of the upper and lower jaws
If you notice any of these in your child, schedule an evaluation sooner rather than later. About 75% of children benefit from orthodontics, and early evaluation is the only way to know whether your child is one of the ones who needs help during the growth years.
10 Key Benefits of Interceptive Orthodontics for Children
This is the core of what parents want to understand. Here are the ten most important benefits of interceptive orthodontics for children, explained in plain language.
1. Guides Healthy Jaw and Facial Growth
A child's jaw is not fully formed. It is actively growing and highly responsive to guidance. This is the single biggest advantage of early treatment.
Early orthodontic intervention leads to significant improvements in dental alignment, occlusion, and skeletal relationships in children. In the case of conditions such as posterior crossbites and Class III malocclusion, evidence-based literature shows that a relatively short phase of interceptive treatment with simple appliances can normalize abnormal growth, and that the result of this treatment approach will remain stable over time.
If jaw problems are left until the growth window closes, typically by the mid-teen years, the only options left may be surgery or prolonged treatment that still cannot fully correct the underlying structure. Acting early, while the jaw is still forming, keeps options open and results better.
2. Creates Space for Permanent Teeth to Come In Properly
One of the most common reasons parents bring their children in is crowding. When there is not enough room in the jaw for permanent teeth, those teeth either come in crooked or get stuck beneath the gum line.
Appliances like palate expanders can gently widen the upper jaw to create the space permanent teeth need. If a child's upper jaw is too narrow, a palatal expander can gently widen it, preventing crowding and crossbites. This approach works with the body's natural growth rather than against it, which is why it is more effective when done during the early mixed dentition phase.
Creating this space early often means fewer teeth need to be extracted later, a benefit most parents are very glad to hear.
3. Corrects Bite Problems Before They Become Structural
Bite problems like crossbites, underbites, and open bites are not just cosmetic concerns. If left untreated during the growth years, they can affect how the jaw develops, how teeth wear down over time, and even the shape of the face.
Studies suggest early intervention may help reduce overjet-related incisor trauma, improve psychosocial well-being, and simplify later treatment phases. When a crossbite or underbite is caught and corrected at age 7 or 8, the jaw can grow symmetrically and correctly. Waiting until age 14 means the jaw has already formed incorrectly, and correction is far more complex.
4. Stops Harmful Oral Habits Before They Cause Lasting Damage
Thumb sucking, finger sucking, and tongue thrusting are normal behaviors in very young children. The problem comes when these habits continue past age 4 or 5, because at that point they can actively push teeth out of alignment and reshape the developing jaw.
Habit appliances used in Phase 1 treatment are designed to gently discourage these behaviors and allow the jaw and teeth to return to a normal development path. Catching this early prevents what would otherwise become a serious structural problem.
5. Reduces or Eliminates the Need for Tooth Extractions Later
Many parents do not realize that one of the main reasons teeth need to be extracted during teenage orthodontic treatment is that there was not enough room in the jaw to begin with. By using expanders and other appliances during Phase 1 to create space, the need for extractions is often significantly reduced or avoided entirely.
Early short-term interceptive orthodontic treatment with simple appliances can efficiently correct certain malocclusions and help to either reduce the complexity or even avoid the necessity of complex and expensive procedures during puberty. That is a meaningful benefit, both for your child's health and your long-term treatment costs.
6. Shortens and Simplifies Future Phase 2 Treatment
A child who goes through a well-planned Phase 1 program does not necessarily skip Phase 2, but their Phase 2 is typically much shorter and simpler. The hard structural work has already been done. Phase 2 in these children becomes a matter of final tooth alignment rather than a years-long correction of jaw and bite problems.
Phase 1 averages 6 to 18 months, followed by a monitoring period. Phase 2, if needed, lasts 12 to 24 months, but early intervention often shortens it. For some children, Phase 2 is not needed at all.
7. Protects Front Teeth from Injury
Children with protruding upper front teeth, sometimes called "buck teeth," face a real risk of dental injury during everyday childhood activities like sports, play, and falls. The reduction in overjet during treatment indicates a correction of anterior tooth protrusion, which may prevent potential dental trauma associated with protrusive incisors.
Bringing those front teeth into a more protected position during Phase 1 is a simple and practical benefit that is easy to overlook until an injury happens.
8. Improves Speech and Breathing Function
The position of the teeth and jaw directly affects how a child speaks and breathes. Children with significant bite issues or narrow palates may develop speech patterns that are difficult to correct later, and they may habitually breathe through their mouths because their airway is restricted.
Interceptive orthodontics enhances bite function, potentially alleviating speech impediments or sleep apnea symptoms. For example, widening the jaw can improve airway space, promoting better sleep. Addressing these issues early, while the jaw is still forming, gives the best chance of a lasting improvement in both speech and breathing.
9. Builds Confidence During the Most Important Social Years
Children between the ages of 6 and 12 are at a stage where social relationships and self-perception start to matter more. Visible dental issues, including protruding teeth, significant crowding, or a noticeably uneven smile, can affect a child's confidence during these years.
Early interceptive orthodontic treatment can make noticeable improvements to a child's appearance at an age when it truly matters to them. A child who feels good about their smile is more likely to smile, more likely to engage socially, and more likely to carry that confidence forward into adolescence.
10. Monitors and Guides Growth Progression Over Time
Phase 1 treatment does not end when the appliance comes off. After active treatment, children typically enter a monitoring phase where the dentist or orthodontist tracks how permanent teeth are coming in and how the jaw continues to develop.
This ongoing observation means that any new issue that develops during the growth years is caught quickly, rather than being discovered at age 14 when it has already become significant. The monitoring period is one of the most underappreciated parts of Phase 1 treatment, and it is included as a standard part of the process at Dr. Leslie Jacobs Pediatric Dentistry.
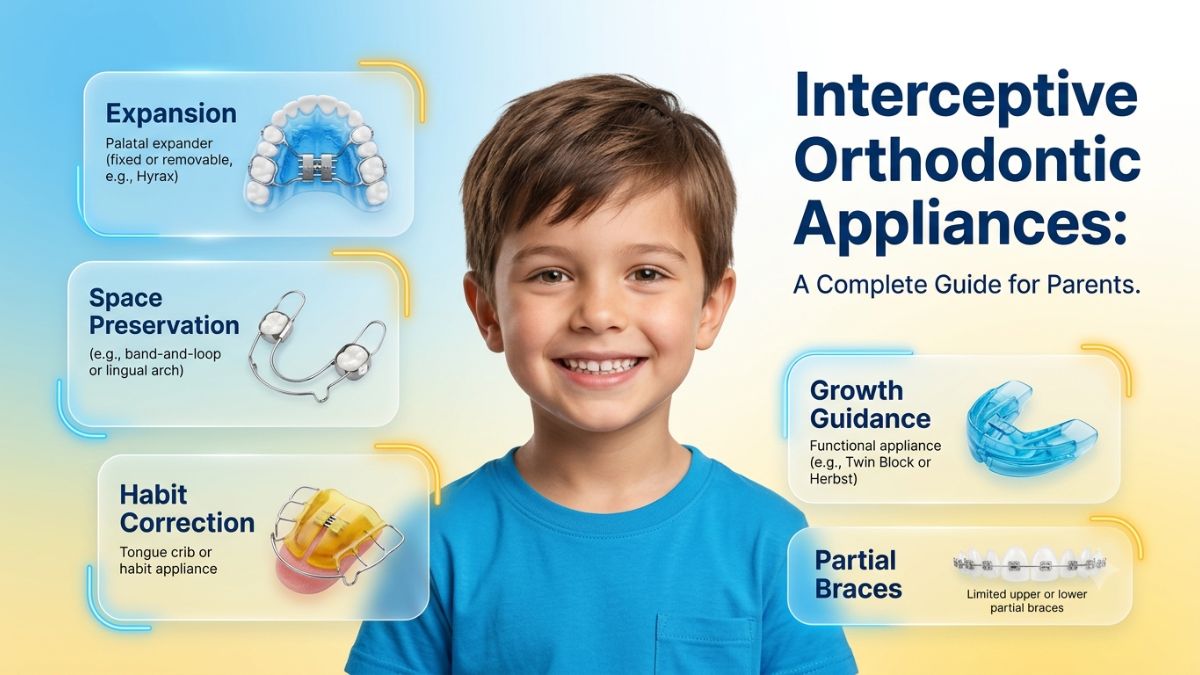
What Appliances Are Used in Interceptive Orthodontic Treatment?
Parents often want to know what Phase 1 treatment actually looks like on a day-to-day basis. Here is a plain-language overview of the most common appliances used.
Palate expander: This is one of the most common Phase 1 appliances. It fits on the roof of the mouth and is activated gradually to widen the upper jaw. The appliance of choice is typically a tooth-borne Rapid Palatal Expander (RPE) which is usually activated once a day for four to six weeks, depending on the severity of the problem, and left in place for 9 to 12 months. Children adjust to it quickly, and most report only mild pressure or a slight lisp for the first few days.
Space maintainers: When a baby tooth is lost earlier than expected, the surrounding teeth can drift into the empty space and block the incoming permanent tooth. A space maintainer is a simple appliance that holds the space open until the permanent tooth is ready to erupt.
Partial braces: Unlike full braces, partial braces are placed on only specific teeth, usually the front teeth, to correct limited but important alignment issues during early childhood.
Habit appliances: These are used to help children stop thumb sucking or tongue thrusting. They do not hurt, but they make the habit less automatic, allowing the teeth and jaw to return to a normal position over time.
Removable plates and retainers: Some children use removable appliances that are worn for a set number of hours each day to guide jaw and tooth development without a fixed device.
Is Treatment Painful?
Most children tolerate Phase 1 appliances very well. There may be mild soreness or pressure for a day or two after adjustments, similar to what you feel after a dental cleaning. Over-the-counter pain relief and soft foods for a day or two are usually all that is needed. Children adapt quickly, and most do not think about their appliance within a week of getting it.
How Long Does Phase 1 Treatment Last?
Phase 1 treatment usually lasts 6 to 18 months, followed by a monitoring period until it is time to evaluate whether Phase 2 is needed. The total active treatment time depends on what issues are being corrected and how well the jaw responds.
What Happens If You Wait? Understanding the Risks of Delayed Treatment
This is one of the most important questions parents ask, and it deserves an honest answer.
For some children, waiting is perfectly fine. Not every child who has an evaluation at age 7 needs to start treatment right away. Some bite issues self-correct as the jaw grows. Some spacing issues resolve naturally as permanent teeth come in. Part of the value of early evaluation is determining which category your child falls into.
However, for children with real structural issues, waiting past the growth window can mean significantly more complex treatment later. Excessive use of early orthodontics without proper patient selection may increase treatment duration and costs, but the flip side is also true: failing to treat appropriate candidates early can lead to problems that require surgery or extensive treatment in adulthood that could have been avoided.
Specific problems that tend to worsen significantly when missed during the growth years include:
- Skeletal crossbites, which can only be fully corrected without surgery if treated while the jaw is still growing
- Class III (underbite) malocclusions, which tend to worsen during adolescent growth, making early interception during the growth phase the recommended approach to gain maximum skeletal effect
- Severe arch length discrepancies that lead to impacted permanent teeth
- Habits like thumb sucking that, if uncorrected, continue to reshape the jaw over years
The key is proper evaluation by a trained professional who can tell the difference between a child who will benefit from early treatment and one who simply needs to be monitored.
When Is Waiting Actually Fine?
Waiting is a reasonable approach when the issue is mild crowding that may self-correct, when the child is very young and the jaw has not yet shown the growth pattern clearly, or when the child is not developmentally ready to cooperate with an appliance. In those cases, a monitoring schedule every 6 to 12 months is exactly the right plan. At Dr. Leslie Jacobs Pediatric Dentistry, we will never recommend treatment that is not clearly beneficial for your child.
How Much Does Interceptive Orthodontics Cost, and Does Insurance Cover It?
Cost is a real consideration for most families, and it is worth understanding what to expect before your child's evaluation.
The cost of Phase 1 orthodontics can vary depending on the complexity of the treatment and the specific needs of the child. It typically ranges between $2,000 and $4,500. The type of appliance needed, how long treatment takes, and the specific issues being addressed all influence the final cost. Your child's evaluation appointment is the right time to get a precise estimate based on their individual needs.
Does Insurance Cover Phase 1 Orthodontics?
Many dental insurance plans do include orthodontic benefits, and those benefits can be applied to Phase 1 treatment. Orthodontic coverage usually pays around 50% of costs up to a lifetime maximum, often between $1,000 and $3,000 per person. It is important to understand that if your insurance has a lifetime orthodontic maximum, using part of it for Phase 1 will reduce what is available for Phase 2. Your dental insurance coordinator can help you understand exactly how your plan works before treatment begins.
Other Ways to Manage the Cost
Flexible spending accounts (FSAs) or health savings accounts (HSAs) can be used to cover out-of-pocket expenses associated with Phase 1 treatment. These accounts allow you to use pre-tax dollars for eligible healthcare expenses, providing additional savings.
Many pediatric dental practices, including ours in Lafayette, also offer flexible payment plans that allow you to spread the cost of treatment over monthly installments rather than paying everything upfront.
It is also worth considering the long-term financial picture. Phase 1 treatment that creates space and corrects jaw alignment early often reduces the complexity of Phase 2 treatment. A shorter, simpler Phase 2 typically costs less and takes less time than a full correction that could have been partially addressed in childhood.
Frequently Asked Questions
At what age should my child have their first orthodontic evaluation?
The American Association of Orthodontists recommends the first evaluation by age 7. At this age, enough permanent teeth have come in for a dentist to assess the bite, jaw alignment, and spacing. If you notice any of the warning signs listed earlier in this article, schedule an evaluation sooner.
What is the difference between Phase 1 and Phase 2 orthodontics?
Phase 1 is early interceptive treatment focused on jaw development and bite correction, typically done between ages 6 and 10. Phase 2 is comprehensive treatment, usually starting around ages 11 to 14, focused on aligning all the permanent teeth. Some children need both phases; some need only Phase 2; and in some cases, Phase 1 is so effective that Phase 2 is minimal or not needed.
Can a pediatric dentist do interceptive orthodontics, or do I need a specialist?
A trained pediatric dentist can evaluate your child and provide many Phase 1 treatments, including appliances and monitoring. At Dr. Leslie Jacobs Pediatric Dentistry in Lafayette, we assess children for early orthodontic concerns as part of our regular care. We will refer to an orthodontic specialist when a case requires it.
How long does Phase 1 treatment last?
Most Phase 1 treatment lasts between 9 and 18 months, followed by a monitoring period of varying length before Phase 2 is evaluated.
Will my child still need braces after Phase 1?
Possibly, but not always. Phase 1 is not designed to do everything. Its goal is to correct structural issues during the growth years. Many children will still benefit from a Phase 2 to finalize tooth alignment, but that Phase 2 is typically shorter and simpler because of the groundwork laid in Phase 1.
Is interceptive orthodontic treatment covered by insurance?
Many dental insurance plans with orthodontic benefits apply to Phase 1 treatment. Coverage varies by plan, and there is typically a lifetime maximum that applies to both phases combined. Check with your insurance provider, and our team can help you understand your benefits at your child's appointment.
How do I know if my child needs early treatment or if we should wait?
The only way to know for sure is an evaluation with a trained pediatric dentist or orthodontist. An evaluation at age 7 gives you the information you need to make a confident decision. In most cases, the answer will be that monitoring is fine. In the cases where early treatment is recommended, you will have caught the problem at the ideal time.
Schedule a Complimentary Interceptive Orthodontics Evaluation in Lafayette
The best gift you can give your child's smile is an early look. Interceptive orthodontic treatment is not about rushing your child into braces. It is about making sure their jaw is developing correctly and that any real problems are caught and addressed while the window for easy, effective correction is still open.
At Dr. Leslie Jacobs Pediatric Dentistry in Lafayette, we take the time to evaluate every child carefully and give parents an honest picture of what their child needs and what can safely wait. We believe in recommending treatment only when it is genuinely beneficial, and we will always explain our reasoning in plain language so you can make the right decision for your family.
If your child is approaching age 7, or if you have noticed any of the warning signs listed in this article, we would love to see them for an evaluation. Contact our Lafayette office to schedule an appointment today.