.png)
Most parents assume braces are a middle school thing. So when your child's dentist mentions an orthodontic evaluation at age 7, it can feel confusing or even a little alarming. Here is the truth: the American Association of Orthodontists (AAO) recommends that all children be screened by an orthodontist at age 7, not because most 7-year-olds need braces, but because a small number of developing problems are genuinely easier to fix while the jaw is still growing. One visit tells you exactly which category your child falls into.
In this guide, you will learn why age 7 is a specific milestone, what signs to watch for, how early treatment actually works, when waiting is perfectly fine, and what to expect if your family comes in for an evaluation at Dr. Leslie Jacobs Pediatric Dentistry.
Why Age 7? The Real Reason Behind the AAO Recommendation
What Is Happening in Your Child's Mouth at Age 7
Around age 7, something important happens in your child's mouth. Their first permanent molars start to come in, and the front permanent teeth begin to replace the baby teeth. This creates what dentists call "mixed dentition," which simply means a mix of baby teeth and adult teeth existing at the same time.
At age 7, your child's mouth shows both baby (primary) and permanent teeth. This stage gives an orthodontist useful clues about future tooth positions and bite development. The jaw bones are still soft and actively growing at this age, which is the key reason early evaluation matters. Once the jaw finishes growing, correcting structural problems becomes significantly more difficult and sometimes requires surgery instead of simple appliances.
What the Evaluation Actually Looks At
In addition to an intraoral exam, orthodontists use panoramic X-rays to check below the surface to look for extra teeth, missing teeth, impacted teeth, or teeth coming into the wrong positions. ( Refference)
A panoramic X-ray gives the dentist a full picture of every tooth, including teeth that have not erupted yet. Many parents ask whether this X-ray is safe for a young child. The radiation exposure from a dental panoramic X-ray is very low, and it reveals information that simply cannot be seen during a standard visual exam. Without it, a dentist may not know that a permanent tooth is growing in the wrong direction until it becomes a much bigger problem.
What "Evaluation" Really Means
Here is what many parents do not realize before the visit: an evaluation is not the same as treatment. Even if your child doesn't need orthodontic treatment at age 7, taking them for their first visit allows the orthodontist to monitor their growth and avoid costly future problems with the jaws or teeth by detecting and treating orthodontic issues at the right time. ( Reference)
After the evaluation, there are three possible outcomes. First, everything looks great and no action is needed. Second, a minor concern is noted and the child returns for monitoring visits every 6 to 12 months. Third, a specific problem is found that genuinely benefits from early treatment. Most children land in the first or second category.
Signs Your Child May Need an Early Orthodontic Evaluation
To determine if your child needs to see an orthodontist, watch for these warning signs. If you notice any of the following, it is worth scheduling a visit sooner rather than waiting for the regular age-7 timeline:
- Crossbite — When your child bites down, do the upper teeth sit inside the lower teeth on one or both sides? Does their jaw seem to shift to one side when closing? This is a functional crossbite, and it is one of the strongest reasons for early intervention.
- Underbite — The lower front teeth sit in front of the upper front teeth. This involves jaw development and tends to worsen if left untreated during the growth years.
- Severe overcrowding — The baby teeth look very crowded together, which often signals that the permanent teeth will not have enough room to come in properly.
- Teeth that stick out significantly — Front teeth that protrude outward are at a higher risk of being chipped or broken from a fall or sports injury. Early treatment can lower the risk of trauma to protruding front teeth.
- Thumb sucking or pacifier use past age 5 — Thumb sucking is perfectly normal in young children. However, if it continues past the ages of five or six, it can start to significantly damage teeth. Prolonged habits like these can push the front teeth forward and narrow the upper jaw.
- Mouth breathing — If your child consistently breathes through their mouth rather than their nose, this can affect how the jaw develops over time.
- Losing baby teeth very early or very late — While some variation is normal, losing baby teeth too early or too late can create problems with the permanent teeth replacing them.
- Teeth coming in at unusual angles — If permanent teeth appear to be erupting sideways, far out of line, or in unexpected positions, an evaluation should not wait.
Many orthodontic issues, such as jaw unevenness or unerupted teeth, are not visible to the untrained eye. An X-ray and exam by a specialist can reveal potential problems that aren't obvious on the surface.
When Early Treatment Is NOT Recommended
This is something most orthodontic websites do not tell you, but it is important for parents to hear. Not every dental issue benefits from early treatment, and starting treatment too soon can sometimes mean going through two rounds of orthodontic work when one carefully timed round would have been enough.
The AAO supports early exams to make a clear plan: treat now if beneficial, or follow with periodic reviews. The following are situations where watchful waiting is typically the better approach:
Mildly crowded teeth with no bite problems. If the crowding is minor and the bite looks healthy, the dentist will usually monitor the situation as baby teeth fall out naturally. Many mild crowding cases improve on their own.
Slightly crooked individual teeth. A single crooked tooth, especially if baby teeth are still present nearby, is usually not a reason for immediate treatment. The dentist will track how the permanent teeth erupt.
Normal spacing between baby teeth. Gaps between baby teeth are actually healthy and normal. The permanent teeth are larger and often fill that space naturally.
Simple overbite with no jaw involvement. A mild overbite where the upper front teeth overlap the lower ones slightly is common and usually addressed during Phase 2 when all permanent teeth are present.
The honest reality is this: if you bring your child in for an age-7 evaluation and the dentist says "let's just watch and check back in a year," that is a genuinely good outcome. It means your child's development is on track and there is no benefit to intervening right now.
What Is Phase 1 Orthodontic Treatment? A Plain-English Guide
When early treatment is recommended for a child, it is almost always what orthodontists call Phase 1 or interceptive treatment. This is not the same as full braces. Phase 1 is a targeted, limited treatment designed to address one specific problem while the jaw is still growing, using the body's own growth process to make the correction easier.
The goal of early orthodontic treatment is to intercept developing problems, eliminate the cause, guide the growth of facial and jaw bones, and provide adequate space for permanent teeth.
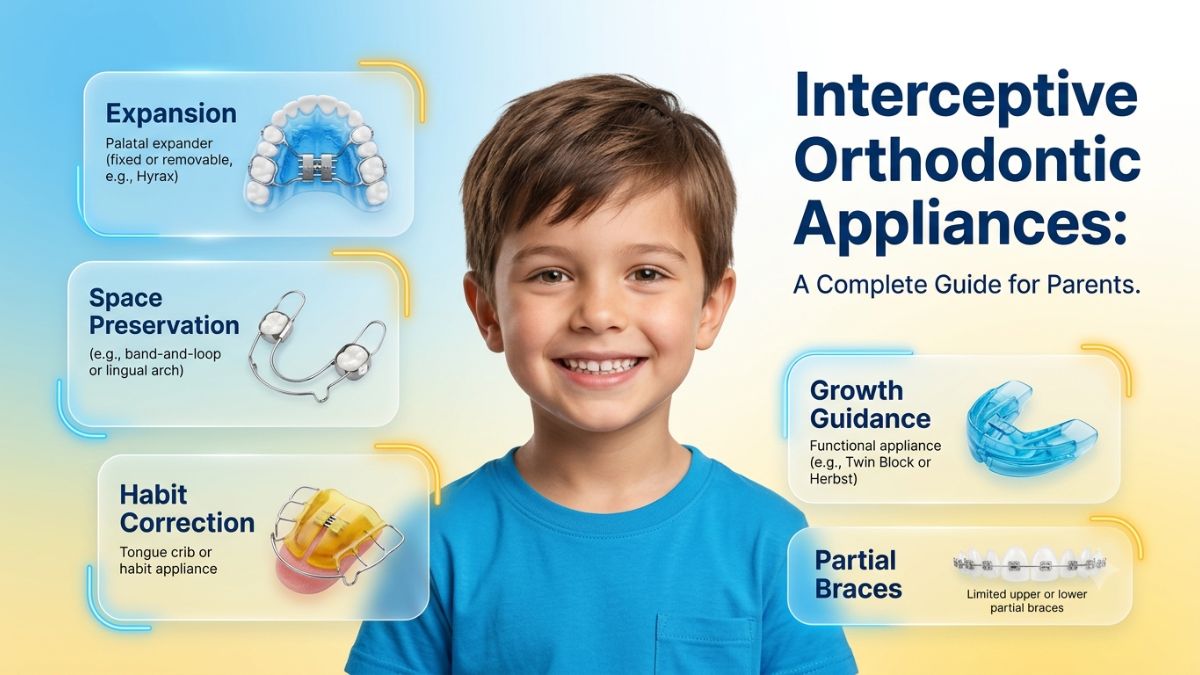
Here are the most common Phase 1 appliances and what each one does:
Palatal Expanders
A palate expander is an oral device used to widen a narrow upper jaw. It is placed along the roof of the mouth and works by gradually pushing the two halves of the palate apart, widening the upper jaw over time. As the palate widens, new bone regenerates and fills the space left behind.
Children and pre-teens are ideal candidates for this treatment because the palate has not yet fully fused. That means the jaw is still responsive to gentle, consistent pressure, and the body does most of the heavy lifting naturally. Once growth is complete and the palate has hardened, this type of non-surgical widening is no longer possible, which is why timing matters so much.
Orthodontists often recommend that children start wearing a palate expander when they are 7 or 8 years old. When your orthodontist starts moving bones this early on, it can reduce the likelihood that your child will need more invasive procedures later in life.
Most children adjust to wearing an expander within a week. Eating and talking feel a little different at first, but children adapt quickly.
Partial Braces
Sometimes a dentist places braces on just the four to six front permanent teeth while baby teeth are still present nearby. The goal is not to straighten every tooth yet but to correct a specific alignment issue, like a crossbite affecting the front teeth, before the remaining permanent teeth arrive. This targeted approach avoids a full set of braces at a young age.
Habit Appliances
For children who are still thumb sucking or tongue thrusting past the age when these habits typically stop, a habit appliance can help. These small, fixed devices remind the child not to place the thumb or tongue in a position that pushes the teeth forward or changes the shape of the developing jaw. They are not painful, and most children adjust within a few days.
Space Maintainers
Space maintainers hold space for adult teeth if baby teeth are lost prematurely. When a child loses a baby tooth too early due to decay or injury, the neighboring teeth can drift into the empty space. This blocks the path for the permanent tooth trying to come in. A simple space maintainer prevents this from happening and is one of the most straightforward Phase 1 interventions available.
How Long Does Phase 1 Treatment Last?
Most patients wear a palate expander for 6 to 12 months, with treatment times varying widely based on the patient's age, the severity of the condition, and compliance. For other Phase 1 appliances, the timeline is similar. After the active treatment phase ends, there is typically a rest period while the remaining permanent teeth continue to come in. During this time, the dentist schedules monitoring visits to assess how things are progressing.
Phase 1 vs. Phase 2: Understanding the Two-Phase Treatment Process
Two-phase treatment means that treatment is done at two different times, often to take advantage of predictable stages of dental development.
Here is a straightforward breakdown of what each phase addresses:
Phase 1 (Ages 7 to 10): Targets a specific structural problem, such as a crossbite, underbite, significant crowding, or harmful oral habit. Treatment uses expanders, partial braces, or habit appliances while the jaw is still actively growing. The goal is not to make the teeth perfectly straight right now. The goal is to create the right foundation.
Rest Period: After Phase 1 ends, the child enters a monitoring period. Baby teeth continue to fall out and permanent teeth continue to erupt. The dentist watches to see how everything settles.
Phase 2 (Ages 11 to 14, typically): Once most or all permanent teeth are in, full orthodontic treatment addresses overall alignment and bite. Because Phase 1 already handled the structural problems, Phase 2 is often shorter and more straightforward than it would have been without early intervention.
A very common parent question is: "If my child has Phase 1 treatment, will they definitely need Phase 2 as well?" The honest answer is that many children do still need Phase 2, but the treatment is usually simpler and shorter. In some cases, Phase 1 fully resolves the problem and Phase 2 is not needed at all. Every child is different, and a personalized evaluation is the only way to know what your child specifically needs.
What Happens If You Skip the Age-7 Evaluation?
For most children, skipping or delaying the age-7 visit does not cause a crisis. If your child does not have any of the warning signs listed earlier, they may be completely fine until their next regular dental checkup catches anything worth noting.
However, for children with specific conditions, timing genuinely matters.
A child with a functional crossbite, where the jaw shifts to one side to bite down, may develop asymmetric jaw growth over time if the crossbite is not corrected early. Scientific evidence suggests that posterior crossbites can benefit from simple but efficient interceptive therapy during the early mixed dentition phase. The same crossbite that an expander can address in several months during childhood may require jaw surgery to correct in adulthood.
A child with significant crowding and early signs of tooth impaction may eventually need permanent teeth extracted to create room, whereas early intervention could have guided the jaw to make space more naturally.
For a child with severe tooth protrusion, waiting increases the time that those teeth are exposed and vulnerable to injury. Early correction can prevent dental trauma and reduce the risk of trauma to anterior teeth, particularly when the anterior teeth are flared out.
The bottom line is this: the age-7 visit is not urgent for every child. But for the children who do have developing issues, catching it at 7 versus 12 or 13 can make a real, meaningful difference in the complexity and cost of eventual treatment.
Frequently Asked Questions About Braces at Age 7
Does my 7-year-old actually need braces?
Most do not. The AAO does not advocate comprehensive orthodontic treatment at age 7. However, interceptive treatment may be appropriate in certain specific situations. The evaluation tells you which situation your child is in. Many parents leave the first visit with nothing more than a plan to check back in 12 months.
My child's teeth look straight. Do they still need an evaluation?
Possibly, yes. Many orthodontic issues, such as jaw unevenness or unerupted teeth, are not visible to the untrained eye. An X-ray and exam by a specialist can reveal potential problems that aren't obvious on the surface. Straight-looking teeth on the surface do not always mean the bite and jaw development underneath are on track.
My dentist referred us to a specialist. Is this really necessary?
If your dentist referred your child, it means they noticed something worth evaluating. It is not an automatic recommendation for treatment. It simply means a specialist should take a closer look. The evaluation itself is informative regardless of the outcome.
Can a 7-year-old use Invisalign instead of braces?
For most Phase 1 issues, fixed appliances like expanders or partial braces are more effective than clear aligners at this age. The structural corrections that Phase 1 targets, such as widening the jaw, require consistent pressure that a fixed appliance delivers more reliably. Your dentist will discuss the best option based on your child's specific needs.
Will my child definitely need braces again after Phase 1?
Not necessarily. Many children do go on to Phase 2 treatment, but it is typically shorter and simpler because Phase 1 handled the foundational issues. Some children complete Phase 1 and require no further orthodontic treatment at all.
Does insurance cover orthodontic treatment at age 7?
Many dental insurance plans include a lifetime orthodontic benefit that can apply to Phase 1 treatment. Coverage varies widely by plan, so calling your insurance provider before the visit is the best approach. We are happy to help families in Lafayette understand their coverage options before committing to any treatment plan.
Is the evaluation painful or scary for my child?
Not at all. The evaluation involves a visual exam, photographs, and a panoramic X-ray. There are no needles, no drilling, and nothing that should feel uncomfortable. At Dr. Leslie Jacobs Pediatric Dentistry, we work at the child's pace and make sure they feel comfortable throughout the entire visit.
What is the difference between a pediatric dentist and an orthodontist?
A pediatric dentist specializes in the overall oral health of children from infancy through adolescence. We are trained to identify orthodontic concerns early and, in many cases, provide Phase 1 interceptive treatment directly. When a case requires comprehensive orthodontic care beyond our scope, we refer to a trusted orthodontic specialist.
Early Orthodontic Evaluations in Lafayette, LA | Dr. Leslie Jacobs Pediatric Dentistry
At Dr. Leslie Jacobs Pediatric Dentistry in Lafayette, we provide early orthodontic evaluations in a calm, child-friendly environment where kids feel comfortable and parents leave with clear, honest answers. Our approach is simple: we look at what is actually happening in your child's mouth, explain what we find in plain language, and recommend only what genuinely benefits your child. We never push treatment that is not needed.
We serve families throughout Lafayette and the surrounding communities, including Youngsville, Broussard, Carencro, Scott, and Duson.
If your child is approaching age 7, or if you have noticed any of the signs mentioned in this guide, we encourage you to schedule a visit. Most children come in, get a thorough evaluation, and leave with good news and a simple monitoring plan. That outcome is just as valuable as catching something that needs treatment, because it gives you confidence that your child's development is on the right track.
Schedule your child's evaluation today. Call our Lafayette office or book online.